-
cameron-is-God.
User deleted
Lateral Slit vs. Sagittal Slit
Dr.Bill Parsley
For at least 4 years, Dr. Wong has tried to talk me in to using lateral incisions. I had experimented with them in the past and found the sites hard to see, hard to transplant, and had problems with popping- so I dismissed it. His results were outstanding and, in 2002, I invited him to write an article in the Hair Transplant Forum. In that article, he pointed out that hairs in a follicular unit tended to line up perpendicular to the exit angle. I focused in close on the donor strip and....he was right! After that, everything started to fall in to place. With lateral sites, the grafts lay more naturally and the curl is correctly aligned. There is no squeeze on the hairs which allows them to keep there separation. I noticed that they make their incisions in a laterally oriented line and, after checking, most donor follicular units tended to line up the same way. It convinced me to give it another try.
Lateral grafting is not new. Several have tried it, but with minigrafts and slots. There was a lot of compromise to the circulation, some necrosis, and it fell out of favor. No one thought that the lateral alignment of hairs in a small unit such as the follicular unit would make much difference- until H&W. However, multiply the effect by 5000 or more and a significance occurs. My fears of circulatory compromise were aided by 1)H&W dense packed with small incisions with no compromise 2)Limmer and Seager, without thinking of the implications, had been using lateral slits, because they were easier to plant, with their stick&place for years with dense packing and outstanding results. With the cut razor blades, the sites are easier to work with and, with experience, popping is much less of a problem for me. The sites are still more difficult to see, but staying in a pattern pretty much corrects that problem.
Also- take the curl. With sagittal sites, the tendency is to put the grafts in so the hairs are aligned parallel with the desired hair angle. Not only do the grafts not seat quite as well, but the curl is 90 degrees off the desired curl angle. Angling is more difficult with the multihaired grafts using sagittal incisons (I still don't think lateral sites make any difference with single haired grafts).
Of course, many centers get wonderful results with sagittal sites. But these technique modifications add up and give better and better results. There is a learning curve, but for someone experienced, it is not too great.
No- I don't work for H&W, but I do recognize good work and progress.
One note about circulation. There is a supragaleal plexus that connects to the subdermal plexus by vessels that run vertically. The subdermal plexus connects via vertical vessels to the subepidermal plexus. A plexus probably looks like a spider web sitting horizontally in the skin. Created sites with sag or lateral blades have to penetrate thru the subepidermal and the subdermal plexus in order to get the bulbs into the fat layer where they naturally lie. If the incisions stops in the dermis the bulbs won't be where they should be, the grafts will be harder to plant, may fold on themselves, or sit to high. The damage to the subdermal plexu with either orientation is probably about the same.
The difference is that a lateral incision will cut thru more of the dermal vessels than a sagittal incision. With larger lateral blades this is definitely significant. Limmer, Seager, and H&W, however, have show pretty well that smaller sites (1.2mm or less) do not cause a problem. It is true that lateral sites do not penetrate as far into the fat layer and are logically less damaging to the the subcutaneous vessels. If one stays above the important supragaleal plexus, the sagittal sites aren't very damaging. This is where tumescence helps.
All in all, this is probably a push and, correctly used, neither orientation should have signficant impact on the circulation. Scientific studies would be helpful here.
-------------------------
Dr.Bill Parsley
Un ulteriore spunto di discussione:
1.)1. Why does the lateral slit method allow increased density of FU packing? Is it really because of the way the FU can be angled to exit the skin Or I am simply confusing FU packing with cosmetic density.
Well, it's actually the opposite end of the angle that makes dense packing easier. You see, when the incisions are made in the recipient scalp they are made at an angle parallel to the native hair growth. This is determined best by buzzing the native hair very short,(2mm to 3mm), so that the hair will not be encumbered by it's own weight. The angle is free to stand at it's natural angle.
When the incisions are made at this angle they are more shallow than had they been made in a saggital manner. A more shallow incision allows for less vascular damage to the recipient scalp which leads to faster healing. More importantly, the nature of the incisions significantly reduces the amount of pressure exherted by the neighboring grafts. The pressure from saggital incisions is cumulative with each additional incision thereby preventing dense packing.
Furthermore, when the Hasson & Wong Lateral Slit Technique is employed the blades that are used to make these incisions are custom cut to the size of the grafts. This means that the incisions are the same width AND depth of the grafts thereby preventing excessive damage to the recipient scalp. When the grafts are inserted into sites that are the same size then there is no risk of compression. When doctors place grafts into sites that are not customized then it is similar to placing a square block into a round hole.
2.) Is this now the 'industry standard' in FU surgery, i.e. should most HT candidates seeking FU transplant of good density (equal to or greater than 40 FU / cm2) in 1 session only go with surgeons offering lateral slit ?
We think so but more importantly go with a doctor that you feel fits your situation the best. Don't get caught up in shear density numbers as they are misleading and may not apply to your situation. One patient that gets 40 per cm2 may look more dense than another that has 60 per cm2 due to his hair characteristics.
Peace,
Joe Tillman
aka, Jotronic
Hasson & Wong
Edited by rummenigge - 6/1/2010, 19:53. -
titty.
User deleted
Chi è ke cortesemente m fa una breve traduzione? per spiegarmi le differenze fra le due tecniche? Non vorrei aver frainteso.. nn me la cavo molto con l'inglese . -
.
Lateral Slit vs. Sagittal Slit (Dr.Bill Parsley)
Ricordo a tutti che questo è un articolo scritto 10 anni fa !
Durante gli ultimi 4 anni il Dr.Wong ha cercato di convincermi a provare la tecnica delle incisioni laterali (lateral slit). Avevo provato ad adottare questa tecnica in passato e avevo trovato difficoltà nel vedere chiaramente i siti riceventi e nell'effettuare gli innesti oltre a problemi con la fuoriuscita delle unità follicolari dovuta al sanguinamento. Per tutte queste ragioni decisi in passato di non utilizzare più la lateral slit. I risultati del Dr.Wong erano incredibili e quindi nel 2002 lo invitai a scrivere un articolo al riguardo. In questo articolo il Dr.Wong mise in evidenza come i capelli di un'unità follicolari tendessero a allinearsi perpendicolarmente alla direzione d'uscita (come si può vedere nell'immagine qua sotto). Per verificare ciò ho analizzato la losanga estratta con grande attenzione e il Dr.Wong aveva ragione ! Dopo questa scoperta tutto è diventato più chiaro. Con le incisioni laterali le unità follicolari si posizionano in modo più naturale e si tiene conto della direzione e degli angoli.
I capelli non si schiacciano tra loro e questo permette di mantenere la loro naturale separazione. Ho notato che Hasson&Wong realizzano le incisioni seguendo un'ipotetica linea laterale e dopo una verifica ho potuto confermare come le unità follicolari in area donante sono allineate nello stesso modo.
Questo mi ha convinto a riprovare ad utilizzare la lateral slit.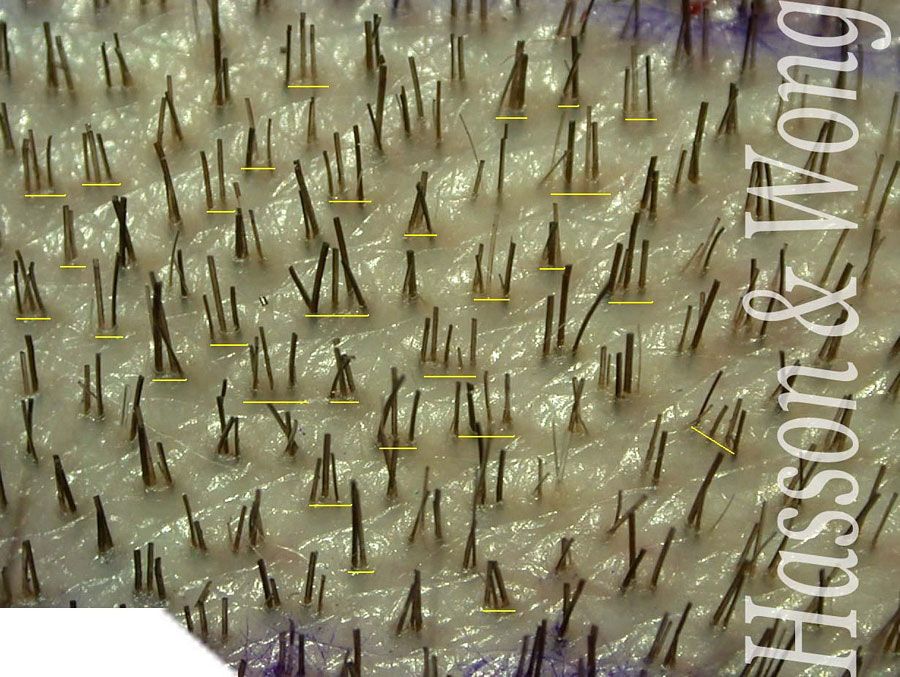
La lateral slit non è una novità. Molti anni fa parecchi chirurghi avevano provato ad usarla ma con i mini-innesti e macro incisioni. Questo aveva portato a seri problemi a livelli di circolazione sfociati alcune volte in necrosi, il che aveva convinto la maggior parte dei chirurghi ad abbandonare la tecnica.
Nessuno aveva pensato che l'allineamento lineare dei capelli nell'unità follicolare potesse fare la differenza fino alla scoperta di Hasson&Wong !
Moltiplicando però questo effetto per 5000 o più è ovvio che ci sia una differenza. Le mie paure di problemi a livello circolatorio sono svanite dopo aver visto che:
1- Hasson&Wong sono riusciti a effettuare interventi ad alta densità con piccole incisioni senza danni a livello di circolazione sanguigna
2 - Limmer e Seager senza pensare alle implicazioni, hanno usato la lateral slit per anni, perchè ritenevano che permettesse una miglior facilità d'innesto attraverso la loro tecnica stick&place, e sono riusciti ad ottenere alte densità e risultati eccellenti.
Grazie all'uso delle lame su misura, è più facile lavorare con i siti riceventi e con un po' di pratica anche il popping (fuoriuscita delle unità follicolari dovuta al sanguinamento) non è più un problema. I siti riceventi sono ancora piuttosto difficili da vedere ma il fatto che seguano un percorso determinato rende di facile soluzione il problema.
Consideriamo ora la direzione. Con l'incisione sagittale si tende a posizionare le unità follicolari in un modo tale da far si che i capelli siano allineati in modo parallelo rispetto all'angolo desiderato. Non solo le unità follicolari non si posizionano facilmente ma l'angolo è di 90° spostato rispetto a quello desiderato. E' più difficile direzionare correttamente le unità follicolari multiple usando le incisioni sagittali (e continuo a pensare che la lateral slit non faccia una grande differenza per le unità follicolari singole).
Senza dubbio moltissime cliniche ottengono risultati fantastici con le incisioni sagittali ma queste modifiche nelle tecniche di incisione apportano costanti miglioramenti e permettono di ottenere splendidi risultati. C'è una curva di apprendimento ma per un chirurgo con esperienza questa non è particolarmente significativa.
Non lavoro per Hasson&Wong ma riconosco il loro buon lavoro e ciò che hanno apportato al mondo dei trapianti.
Una nota aggiuntiva riguardo la circolazione sanguigna. Esiste un plesso supra galeale che si connette con il plesso subdermico attraverso vasi sanguigni che corrono in modo verticale. Questo plesso subdermico si connetta attraverso vasi sanguigni verticali con il presso subepidermico. Un plesso assomiglia a una ragnatela posizionata orizzontalmente nella pelle. Quando si creano i siti riceventi con incisioni laterali o sagittali la lama deve penetrare attraverso il plesso subepidermico e subdermico per far si che i bulbi si posizionino nello strato grasso dove si collocano in natura.
Se l'incisione si ferma a livello del derma i follicoli non saranno dove dovrebbero essere, le unità follicolari saranno più difficili da innestare e potrebbero ripiegarsi su se stesse o posizionarsi troppo in alto. Il danno che si produce a livello di plesso subdermico è probabilmente lo stesso con entrambe le tecniche d'incisione.
La differenza è che l'incisione laterale a mio parere provocherà la recisione di più vasi sanguigni a livello del derma rispetto all'incisione sagittale.
Questo costituirebbe un problema se si usassero lame per le incisioni laterali di grandi dimensioni. Limmer, Seager e Hasson&Wong tuttavia hanno mostrato che creando piccoli siti riceventi (con incisioni minori a 1.2 mm) non si crea nessun problema a livello circolatorio. E' inoltre vero che la lateral slit permette di creare incisioni che non penetrano così in profondità nello strato grasso e causano quindi meno danno a livello vascolare subcutaneo.
Se il chirurgo rimane però sopra l'importante plesso supragaleale anche la tecnica d'incisione sagittale non provoca molti danni. In questo caso la tumescenza (ottenuta attraverso l'uso di soluzione salina) è di grande aiuto.
Per concludere a mio parere, se correttamente usata, nessun tecnica di incisione dovrebbe provocare un effetto significativo a livello di circolazione anche se alcuni studi scientifici potrebbero essere utili.
-------------------------
Dr.Bill Parsley.
LATERAL SLIT VS SAGITAL SLIT |

